


Which Health Care Provider Will You Get?
Healthcare Provider Selection and Patient Care


THE PATIENT JOURNEY
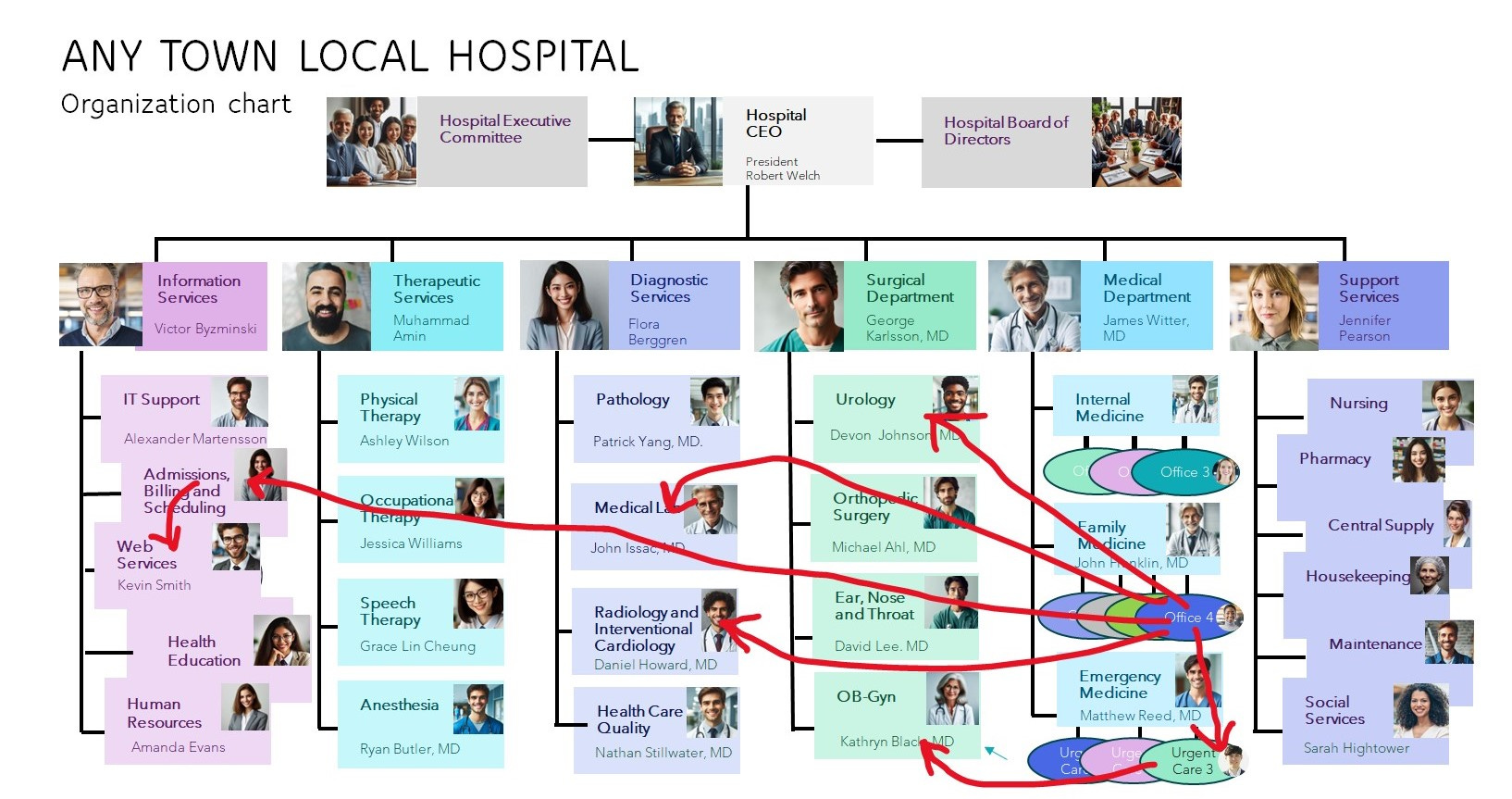
The 24-year-old patient with recurring urinary tract symptoms was repeatedly treated by the health care system for her recurring problem as if it were a new illness. Each time she sought care, she went through the same intake process and saw a different provider, resulting in delayed, fragmented care, and inconsistent treatment. Her healthcare cost was $10,000 for a diagnosis that should have been made for $100.
How Emergency Rooms Match the Right Patient to the Right Provider at the Right Time
Regrettably, most of our healthcare system fails to differentiate between various health conditions as defined by Clayton Christensen and discussed in Which Provider Do You Need when determining which provider should treat a patient. There is one exception: the Emergency Department, also known as the E.R. In the E.R., patients are initially seen and triaged by experienced clinical personnel to assess their level of acuity or how urgently they need care before a critical event occurs. Bad things sometimes happen quickly in an ER so time to treatment initiation (TTI) is critical. This triage process essentially involves making repeated assessments about the severity of the patient’s illness and plan actions for the patient based on the assessment.
Patients are seen in order of severity. The ER doctor evaluates the patient to determine whether they can manage the case in the Department or if an admission is necessary. This triage system helps sort patients for appropriate and timely care, from a cast application to stabilization with intravenous (IV) fluids until the patient can be transferred to the operating room for surgical management.
Why Do Medical Offices Assign the Patient to the Wrong Provider at the Wrong Time?
In ambulatory care clinics operated by a local hospital, limited triage is undertaken. The message on hold says, “If this is an emergency, hang up and call 911.” The reason for that message is that when a patient calls the receptionist pool, these personnel lack medical training. In most instances they are not located in the medical office or even in the same town. They function simply to fill the schedule for the patient’s regular physician, so the only appointment is often weeks away. If the patient cannot wait, they are offered an appointment with a more available, but usually less experienced provider (paid a lower salary). A sick or anxious patient will usually choose the first available provider unaware of the differences in medical training and experience.
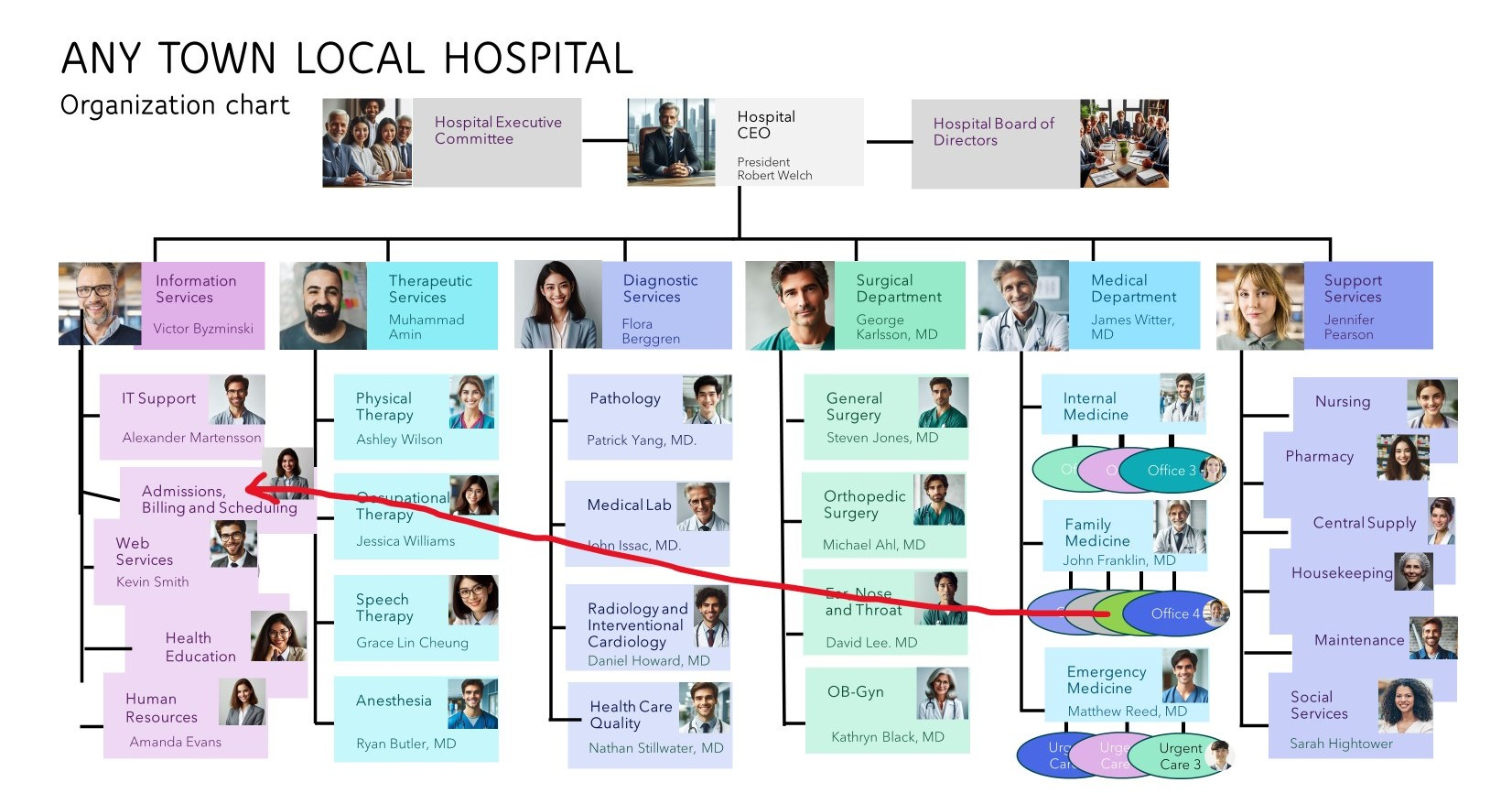
For patients with undiagnosed, complex conditions, the least trained provider may not be the best choice for care of the patient. Less experienced providers may lack confidence in diagnosing based on clinical history alone, leading them to order tests, X-rays, and refer patients unnecessarily to specialists.1 This approach not only delays diagnosis and treatment but also increases costs.2 Patients with complicated conditions, Christensen’s Solution Health, will experience delays because all of the scheduling is done only through the non-clinical Scheduling Department. Because the patient’s regular doctor has no availability by system design, the patient may be referred to a consultant who might not be the correct specialty.
In contrast, an experienced clinician typically takes a thorough history which can be augmented with artificial intelligence patient interviewing.3 Next, they perform a physical exam to arrive at an accurate diagnosis without extensive testing. This leads to prompt treatment initiation, often resolving the issue in a single visit. The follow-up can occur through virtual e-visit technology, minimizing costs of care and improving outcomes for the patient.
When patients present with complex or undefined illnesses, the practitioner's expertise becomes crucial. While apprentice-like training is adequate for managing simple or common conditions, extensive academic education is necessary to recognize and treat illnesses that less experienced providers might not be familiar with or have minimal experience handling.
As discussed in Episode 2, we know most illnesses resolve without any medical involvement. In a small number of illnesses medical intervention will prevent significant illness or death. In these instances, training matters.
When Is Treatment Needed?
Time to treatment initiation (TTI) is an important concept to understand about healthcare. TTI is the interval of time between onset of symptoms, or suspicion of disease and initiation of therapy; being a combination of wait times for consultative, diagnostic, and treatment services. Time to treatment initiation (TTI) has previously been associated with an absolute increased risk of death. TTI is important in patients presenting with a condition like new onset angina because they have a >1% risk of sudden death awaiting definitive diagnosis by catheterization and treatment by coronary bypass grafting.4 In cancer delays in treatment can increase death from 1.2% to 3.2% per week.5 A 30% increase in mortality after waiting two months for care is very significant. Waiting for appointments while going from one consultant to a test to an X-ray to another consultant for a procedure or different test can affect your health outcomes. An upcoming discussion will show how the process of care should be rendered for the best results.
Opinion:
Only ER care is individualized to the patient. Other healthcare takes an across-the-board approach as if each clinical presentation is a unique episode of sickness to be managed without regard to the patient’s history, social environment or context.
From a health system administrator’s perspective, the one-size-fits-all approach is financially advantageous. Using the least experienced providers for initial care is perfect. They are paid lower salaries and benefits packages, and their propensity to order more tests and referrals generates additional revenue for the system. This comes at the cost of quality of care, as the focus shifts from the patients to the profit.
Matching the right patient to the right provider, as seen in the ER model, could improve outcomes and reduce costs, but it requires a shift in how healthcare is delivered and prioritized. It requires health systems to invest in technology to aid their best clinicians.
Instead of a healthcare system, we have a sick care system. The system is functioning as designed.
Preview
The next Episode will describe how the health system works in detail. We will discuss how insurance pays for visits, not talking to patients and thinking about the diagnosis and never for researching the best care plan. The ideal workflow for organizing healthcare will be discussed in the Analysis of Case #1.
Case #2 will question why health systems actually make more money from poor quality care than from optimal outcomes.
Anderson AM, Matsumoto M, Saul MI, Secrest AM, Ferris LK. Accuracy of Skin Cancer Diagnosis by Physician Assistants Compared With Dermatologists in a Large Health Care System. JAMA Dermatol. 2018 May 1;154(5):569-573. doi: 10.1001/jamadermatol.2018.0212. Erratum in: JAMA Dermatol. 2018 Jun 1;154(6):739. doi: 10.1001/jamadermatol.2018.2035. PMID: 29710082; PMCID: PMC6128496
Vinas F, Ben Hassen I, Jabot L, Monnet I, Chouaid C. Delays for diagnosis and treatment of lung cancers: a systematic review. Clin Respir J. 2016;10(3):267-271. doi: 10.1111/crj.12217