
Why Are Doctors Ordering So Many Tests?
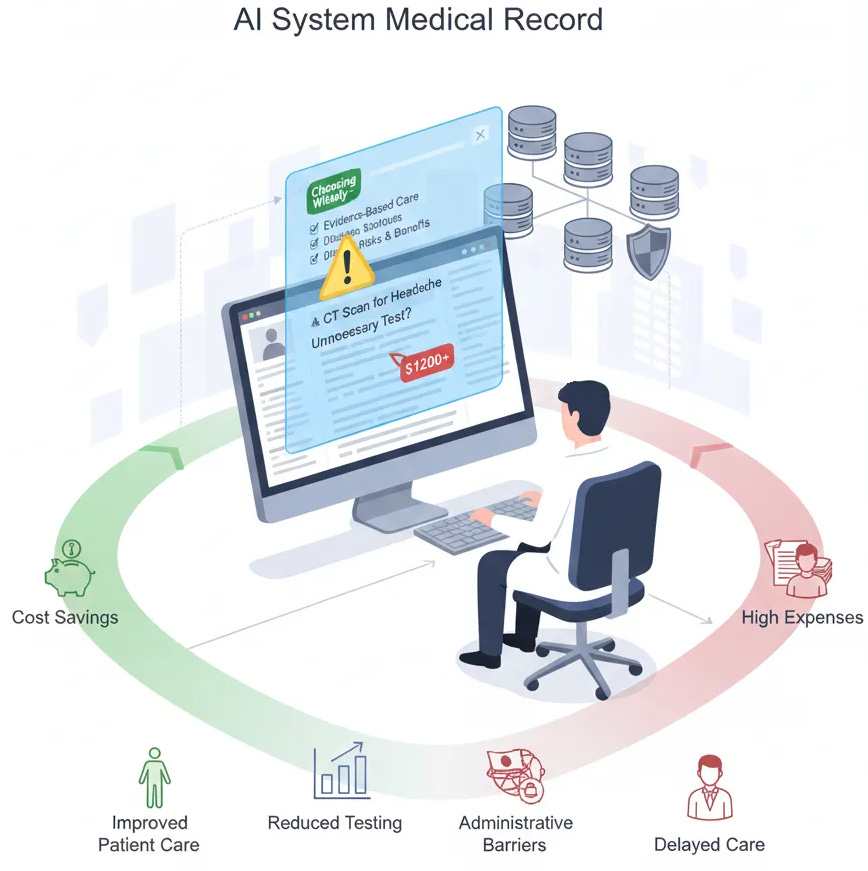
Could an AI-assisted Electronic Medical Record help?

Medical testing is a critical tool in diagnosing, treating, and monitoring patients, but the rise in the number of tests being ordered has raised concerns about cost, patient safety, and the overall value of care. What is over-testing? How can over-testing be reduced?
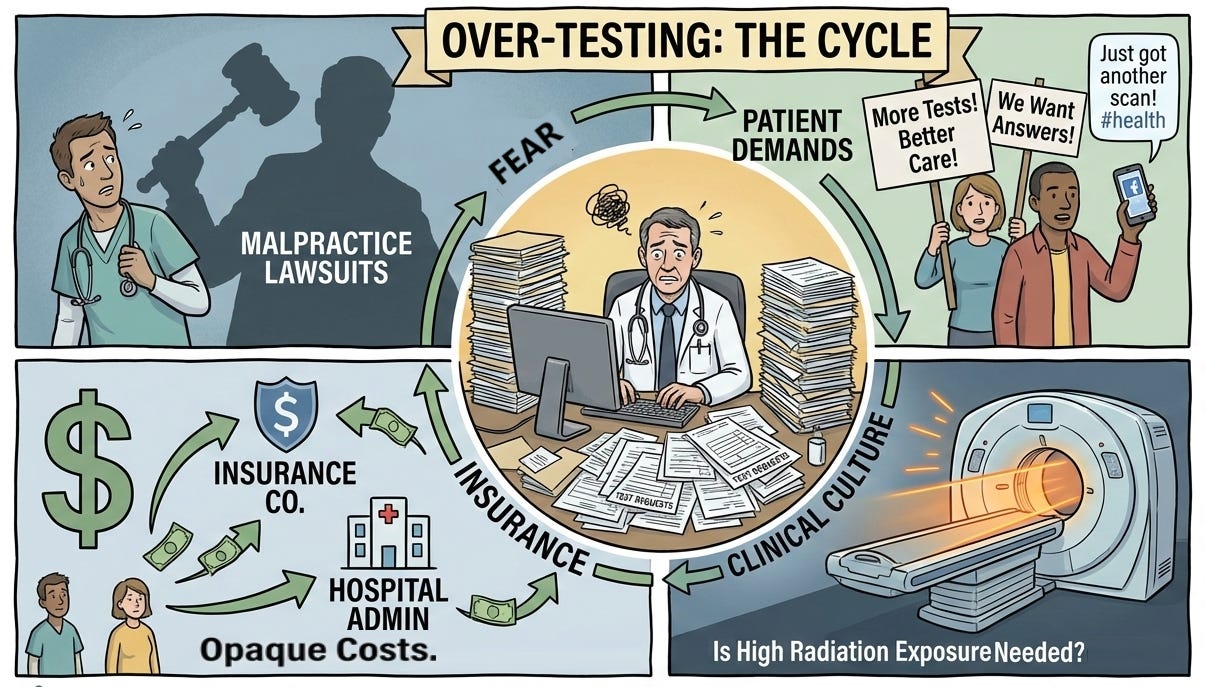
The Fear Factor
Lawsuits are the root cause of doctors ordering too many diagnostic tests. We have discussed how defensive medicine, the fear of being sued, affects medical decision-making as discussed in Treat the Patient or Avoid a Lawsuit? It is the primary motivation behind doctors’ decisions to overtreat as explained in Malpractice Fear Drives Overtreatment. This practice results in overuse of medical resources and unnecessary costs.
The Illusion of Thoroughness
A second key driver of testing is the culture of modern medicine, which often equates more testing with better care. This is actually motivated by litigation concerns, though rationalized as improved care. As I admitted in Was I Guilty of Malpractice I convinced myself the hematology machine was better care after the attorney asked me why I did not order a white blood count for the diverticulitis patient. Was it really better care? How would we know? Unless every case of abdominal pain presenting to a doctor’s office anywhere is studied for the outcomes, we will never know. Providers do not allow aggregation of patient data, even if de-identified, citing the Health Insurance Portability and Accountability Act (HIPAA) to prevent researchers from evaluating which tests are beneficial or unnecessary.
Facebook Medicine: Social Influence in Patient Expectations
Finally, patients drive over testing. Patients often expect, or even demand, comprehensive testing as a sign of thoroughness and quality. Ordering tests has taken the place of doctors spending time discussing diagnoses and treatment plans with patients. Previously, when insurance offered less outpatient coverage and patients paid for tests themselves, discussions about necessity were common and patients often chose to delay testing due to cost. If the doctor thought it essential, they could usually convince the patient to pay for it. Today, insurance conceals test costs from both doctors and patients, so with no personal financial consideration, tests are ordered more freely. People get health information from Social Media.
The AI Chatbot Doctor
Patients use LLMs for medical advice. Entering only some symptoms without others or omitting pertinent negatives into an AI chatbot can lead to erroneous results. Insufficient context and omitted diagnostic steps may lead to the suggestion of extensive investigations of easily ruled-out conditions. A patient reading a structured AI differential diagnosis can think the AI chatbot is smarter than their doctor.
The Lost Art of Patient Education
There is a disincentive for the doctor to disagree with the patient who demands a test. For example, if a neighbor has been referred to a neurologist and had a CT scan for a headache, patients think everyone should have the same thorough work-up. Any doctor not doing it must not be thorough or not care about their patients and will be discussed on Facebook. A tension headache is better addressed with an exercise program, but the patient may demand a CT-scan. The time required for a primary care doctor to explain that the patient does not need a CT scan is considerable. There is an adage in medicine, “Nobody pays for patient education.” Taking the time to explain how a CT scan is not like a plain X-ray but rather contains a great deal more radiation requires patience. The doctor must first inquire why the patient believes they need a CT scan and debunk misinformation. Then they have to explain the following diagram.
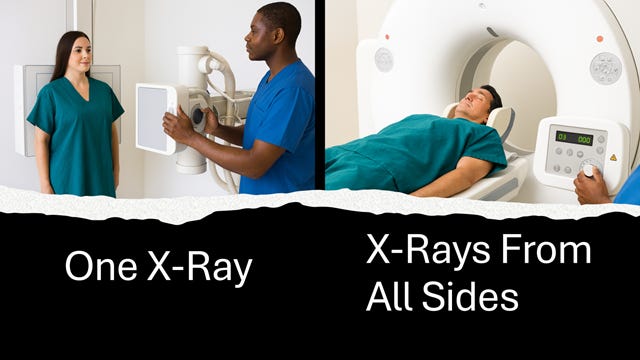
The average person in the U.S. receives about 3 mSv per year from natural sources. A CT scan of the abdomen with contrast (~8 to 15 mSv) delivers the same radiation dose as approximately 80 to 150 plain abdominal X-rays (~0.1 to 0.2 mSv) or 5 years of life. No one knows the risk of repeated CT scans but radiation risk is cumulative throughout life.
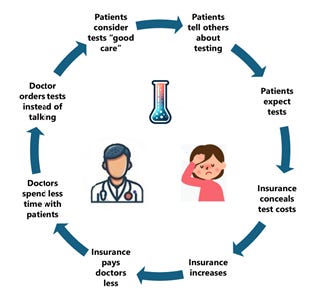
How Insurance Companies Fuel the Cycle of Excessive Testing
Today, the explanations to patients are abbreviated because the insurance motto is, “Doctor, we pay you to see the patient (volume). If you want to practice quality medicine, do it on your own time.” Since neither the doctor or the patient know what the cost of the testing actually is, the easiest option is to simply order the test. Over testing continues to increase because many insurers profit based on a percentage of the total bill. Insurance companies compensate by decreasing the CPT code values paying the doctor less as discussed in How Do Health Insurers Raise Costs. Instead of talking to the patient and educating the patient about the need for tests, the doctor has less time to ask questions to establish the diagnosis and orders more tests as a substitute for time with the patient. The cycle repeats itself as shown in the diagram below.
False Positives, Real Consequences: Anxiety, Inconvenience, and Risk
Moreover, the overuse of diagnostic tests is not without consequences. Financially, the healthcare system bears a significant burden when unnecessary tests are performed. Access is denied to patients who truly need testing. The dramatic rise in healthcare costs are passed on to patients as higher insurance rates or lower wages. For patients, excessive testing can lead to anxiety, inconvenience, and even physical harm. False positives or incidental findings may result in further invasive procedures, exposing patients to additional risks without clear benefits.
Attempts at Change
To address over testing, a rudimentary initiative, “Choosing Wisely” campaign recommends avoiding specific tests, treatments, and procedures that provide minimal clinical benefit in particular clinical situations. The campaign has grown to include over 600 recommendations from more than 70 medical specialty societies, covering a wide range of low-value services. The recommendations target imaging studies (26.8%), laboratory tests (24.9%), medications (22.7%), and procedures (17.9%). Recommendations focus on services used for treatment (39.3%), diagnosis (30.2%), and screening (17.7%).1
Examples of Specific Recommendations To Avoid Low Value Care
Diagnostic imaging:
Avoid imaging for uncomplicated headaches
Avoid cardiac imaging in patients without cardiac history
Avoid preoperative chest x-rays in patients with unremarkable history and physical examination
Avoid low back pain imaging without red-flag conditions (e,g, numbness, urinary symptoms, history of cancer, fever, trauma with neurologic symptoms).
Laboratory testing:
Avoid population-based vitamin D screening
Avoid triiodothyronine (T3) testing for monitoring hypothyroidism (use TSH instead)
Avoid HPV testing in women younger than 30 years of age.
Medications:
Avoid antibiotics for acute sinusitis
Avoid prescription NSAIDs (ibuprofen, Advil™) in patients with hypertension, heart failure, or chronic kidney disease.
Pulmonary medicine:
Avoid CT surveillance of indeterminate pulmonary nodules more frequently than guideline recommendations
Avoid CT screening for lung cancer in low-risk patients
Avoid chest CT angiography for pulmonary embolism in low-probability patients with negative D-dimer.
Critical care:
Avoid routine daily diagnostic testing without specific clinical questions
Avoid red blood cell transfusion in stable ICU patients with hemoglobin >7 g/dL
Avoid deep sedation without daily lightening attempts
The “Choosing Wisely” campaign emphasizes patient-physician conversations about when these services are—and are not—indicated.2
Opinion
All of the recommendations of the “Choosing Widely” campaign could be integrated as an AI agent inside today’s electronic medical record systems used by nearly every physician ordering tests. A warning could appear when they placed a questionable order, like a drug interaction warning. CT scans for headaches (CPT code 70450) is an example of a wasteful order. In Florida it costs $7590.3 It’s easy to understand why hospital administrators would not pay for software so doctors wouldn’t order expensive (profitable) tests. ”Choosing Wisely” is a set of reasonable evidenced-based suggestions, not requirements. Simply requiring these recommendations for Medicare reimbursement would make this happen.
Health data is scattered throughout thousands of disparate electronic health records (EHR) databases protected from the public under the ruse of patient privacy (HIPAA). The manufacturers of EHRs could facilitate this health data being aggregated for research if the Office of the National Coordinator for Health IT (ONC) demanded it because ONC certifies these systems.
The Centers for Medicare and Medicaid Services (CMS) could allow access to de-identified information in the Medicare database that would permit researchers to analyze effective tests, investigations, and treatments using modern big data tools. Hospital lobbyists spend $20-$25 million dollars annually lobbying Congress to avoid these attempts at transparency that would reduce waste, over-testing, overtreatment and over charging.
The health system is functioning as designed. This situation will remain the same until we break the cycle by creating a system focused on doctors and patients rather than on corporations and profits. Achieving this will depend on lawmakers adopting new perspectives on payment for healthcare, tort litigation, patient safety and access to care or electing different representatives.
Conclusion
In conclusion, while doctors do sometimes order too many tests, the reasons are complex and multifaceted, but all have a common origin in litigation avoidance. Balancing thoroughness with prudence is a challenge in modern healthcare. By fostering a culture of critical thinking, transparency, and patient-centered care, the medical community can reduce unnecessary testing while maintaining high standards of diagnosis and treatment.
Preview
The next essay will show a Case study in how testing should be ordered with questions along the way to ask your doctor to avoid over testing.
Longitudinal Content Analysis of the Characteristics and Expected Impact of Low-Value Services Identified in US Choosing Wisely Recommendations. Ganguli I, Thakore N, Rosenthal MB, Korenstein D. JAMA Internal Medicine. 2022;182(2):127-133. doi:10.1001/jamainternmed.2021.6911.
Engaging Physicians and Consumers in Conversations About Treatment Overuse and Waste: A Short History of the Choosing Wisely Campaign. Wolfson D, Santa J, Slass L. Academic Medicine : Journal of the Association of American Medical Colleges. 2014;89(7):990-5. doi:10.1097/ACM.0000000000000270.
HospitalPriceDB - the database of hospital costs accessed December 28, 2025